



SPARTANBURG, SC – As a retired emergency room doctor and hospitalist in rural South Carolina, I have been following the endless contradictions and flip-flopping of our CDC officials like many others for what seems to be an eternity at this point. In Part 1 of this article I will attempt to clarify the salient features of what I believe to be the most glaring aspects of what these officials have tried to sell to the public and how their narrative has crumbled with each new false iteration of their story.
— Sister Mary Saint Jane always told us as schoolboys, don’t lie, you will need to tell more lies to cover up your previous lies, and then sooner or later it will all come tumbling down.
Americans were ravaged by the winter of 2020 with hundreds of thousands of COVID deaths. There was widespread panic and hysteria that permeated every nook and cranny of the nation. Something interesting happened near year’s end. A Doctor Genevieve Briand at Johns Hopkins University looked at the CDC death data up to Nov 20, 2020. Her initial analysis showed no great deviations from 2019 or 2018. A closer look at the data by causes and by age groups revealed the following: There seemed to be no great conflagration in death numbers, yet the mainstream media was reporting quite the opposite. A closer look at the data revealed the following: the top four leading causes of death in the elderly decreased for the first time in U.S. history, the decrease nearly matching the increase in “reported COVID deaths” by CDC officials.
We need to recognize that about 2.8 million people die every year from various well-characterized known causes, and that these deaths are “normal” meaning they are mostly expected as they are predominately in the elderly and are of the most usual causes. The top category is cardiovascular disease which saw the steepest decline, and those would be heart attack deaths, and strokes and congestive heart failure deaths primarily, then followed by “lung” or pulmonary deaths, meaning bacterial and viral pneumonias and emphysema deaths primarily. The other causes like cancers, sepsis, and infections of all sorts and “’other” had less dramatic declines but declines none the less.
Dr. Briand’s article was immediately pulled within 24 hours by Johns Hopkins officials. Someone though, a stranger to me but a person with integrity, moral fiber, and courage I am sure, archived her data. Yanni Gu has re-posted her original archived data with excellent analysis and commentary, while Ethan Yang has published an accompanying article which is also a very readable synopsis of Dr. Briand’s findings. [New Study Highlights Alleged Accounting Error Regarding COVID Deaths – AIER]
As winter came COVID deaths surged and we entered 2021, The nation reached many horrific milestones proclaimed by the lamestream media. The CDC reported that we had crossed 300, then 400, then 500, then 600,000 COVID deaths. But other courageous people had begun to question the narrative. The Colorado rural county coroner asked why people with gunshot wound deaths over the past year in the state were attributed to COVID. Why did that 17 year old riding his motorcycle at 80 mph then hit a tree and died in the emergency room count as a COVID death. Why was he tested in the first place? Why did that man with end stage cancer who died count as a COVID death? On and on.
We now see the CDC again flip flopping. First, they said, “well it’s really 90% died ‘with’ COVID and 10% died ‘from’ COVID.” This has now morphed with the latest iteration as “95% have died ‘with’ COVID and 5% ‘from’ COVID. This equates to 30,000 COVID deaths from the entirety of 2020 and 2021 to date. Where did the other 570,000 come from? Why not even a year ago a few hundred thousand deaths went missing. How can this be reconciled?
It is interesting to note that the reported deaths now representing a small numerator, divided by an enormous denominator of “positive cases” and potential positive cases or “exposures” as calculated by “surveillance data” give a mortality rate near or lower than the Influenza A rate of 0.1%. So, it turns out that this COVID virus supposedly killed that number of mostly elderly people with many of the usual pre-existing conditions, normally seen in a rather mild typical influenza season.
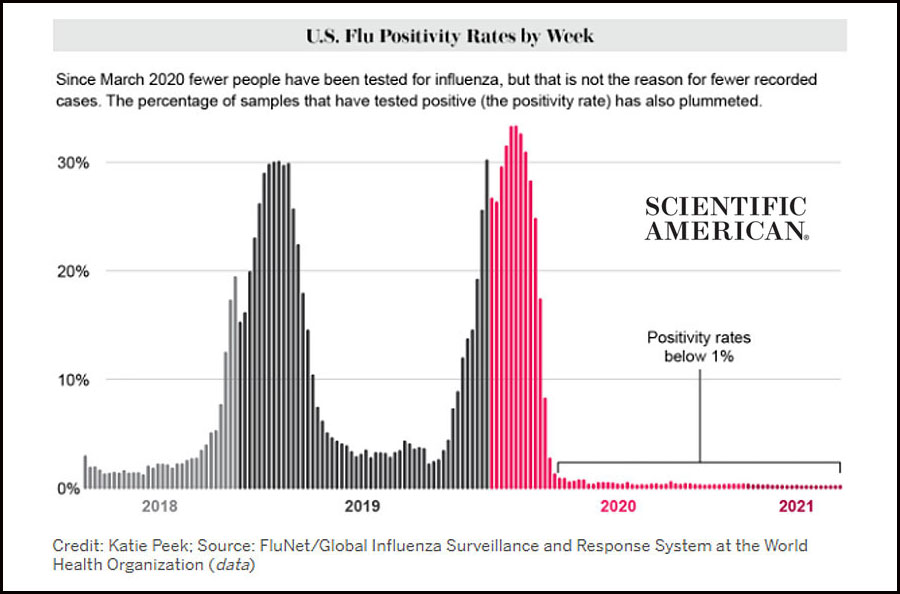
There is another problem. Influenza has been with mankind throughout the ages. It is ubiquitous and cannot just disappear from the face of the earth. The 2020-2021 season saw about 700 Influenza deaths. It is interesting that these 30,000 COVID deaths are similar in magnitude to what we see here in the U.S. during a relatively mild Influenza season. How can this be rationalized?
I believe the answer lies in the way the authorities have used the COVID PCR test for diagnostic purposes, and even whose creator states it was never intended to diagnose illness. Engelbrecht and Demeter state “the intended use of the PCR test was, and still is, to apply it as a manufacturing technique, being able to replicate DNA [and RNA] sequences millions and billions of times, and not as a diagnostic tool to detect viruses.” Because of this extreme sensitivity, it can detect with amplification even the smallest fragments of RNA, “but it cannot determine where these fragments came from,” the authors state. This prescient view has been confirmed by the CDC. The mainstream media itself now reports that the CDC has revealed they are withdrawing from the market by years end the current covid PCR test as it cannot differentiate COVID RNA fragments from Influenza viral fragments and perhaps other cold virus fragments. Dr. Fauci himself has stated, and I paraphrase, that using a high replication rate of 37 or 40, rather than the usual 24 to 30, can make it difficult for an operator in the field to ascribe meaning to a positive result. He frankly stated any iterations above 35 produce meaningless results. Take a penny and double it every day for a month and you will have five million dollars but double it for 40 days and you have five billion dollars. This principal applies here. A more detailed analysis of these concepts can be found in this E-text. Part 2 of this essay will deal with these more complex principles.
In conclusion, there is one thing that is now quite obvious to me, and that is that Sister Mary St. Jane was right then, and she is still right now.
Comments are closed.